Red Scaly Patch On Shin
Overlap syndromes. Occasionally, lichen planus is known to occur with other conditions. For example: Lupus erythematosus overlap syndrome. Lesions of this syndrome.
Circular Red Rash

Lichen planus affecting the shins.
Lichen planus LP is a disease of the skin and/or mucous membranes that resembles lichen. The cause is unknown, but it is thought to be the result of an autoimmune process with an unknown initial trigger. There is no cure, but many different medications and procedures have been used to control the symptoms.
The term lichenoid reaction or lichenoid lesion refers to a lesion of similar or identical histopathologic and clinical appearance to lichen planus i.e. an area which looks the same as lichen planus, both to the naked eye and under a microscope. 1 2 Sometimes dental materials or certain medications can cause a lichenoid reaction. 1 They can also occur in association with graft versus host disease. 1 3 :258
Contents
1 Classification
1.1 Site
1.2 Pattern
1.3 Overlap syndromes
2 Signs and symptoms
2.1 Cutaneous lichen planus
2.2 Mucosal lichen planus
2.2.1 Oral lichen planus
3 Causes
4 Diagnosis
4.1 Histopathology
4.2 Differential diagnosis
5 Treatment
5.1 Cutaneous lichen planus
5.2 Oral lichen planus
6 Prognosis
7 Epidemiology
8 History
9 Notes
10 References
11 External links
Classification edit
Lichen planus has been described as an autoimmune disease, 4 a dermatosis, 5 a papulosquamous disorder, a mucocutaneous disease, 6 and an inflammatory disease. 7
Lichen planus lesions are so called because of their lichen-like appearance 8 and can be classified by the site they involve, or by their morphology.
Site edit
Lichen planus may be categorized as affecting mucosal or cutaneous surfaces.
Cutaneous forms are those affecting the skin, scalp, and nails. 5 6 9
Mucosal forms are those affecting the lining of the gastrointestinal tract mouth, pharynx, esophagus, stomach, anus, larynx, and other mucosal surfaces including the genitals, peritoneum, ears, nose, bladder and conjunctiva of the eyes. 7 10 11
Pattern edit
Lichen planus lesions can occur in many different forms:
Lesion morphology
Description 12 13
Annular
Ring-shaped lesions that develop gradually from single small pigmented spots into circular groups of papules with clear, unaffected skin in the center. Annular lesions occur in approximately ten percent of lichen planus cases. The ring-like lesions may very slowly enlarge, co-join and morph into larger irregular serpentine bands, sometimes accompanied by lines See Linear, below.
Linear
Papules are arranged in a line the Blaschko line. 14 This pattern may develop secondary to trauma koebnerization or, uncommonly, as a spontaneous, isolated eruption, usually on the extremities, and rarely on the face. 15
Hypertrophic
This pattern usually occurs on the extremities, especially the shins and the interphalangeal joints, and tends to be the most pruritic variant of lichen planus. Also known as Lichen planus verrucosus.
Atrophic
This morphology is characterized by the presence of a few well-demarcated, white-bluish papules or plaques with central superficial atrophy. This is a rare variant of lichen planus.
Bullous
This morphology is characterized by the development of vesicles and bullae with the skin lesions. This is a rare variant of lichen planus, and also known as Vesiculobullous lichen planus.
Ulcerative
This morphology is characterized by chronic, painful bullae and ulceration of the feet, often with cicatricial sequelae evident. This is a rare variant of lichen planus.
Pigmented
This morphology is characterized by hyperpigmented, dark-brown macules in sun-exposed areas and flexural folds. This is a rare variant of lichen planus.
Overlap syndromes edit
Occasionally, lichen planus is known to occur with other conditions. For example:
Lupus erythematosus overlap syndrome. Lesions of this syndrome share features of both lupus erythematosus and lichen planus. Lesions are usually large and hypopigmented, atrophic, and with a red-to-blue colour and minimal scaling. Telangectasia may be present. 13 16
Lichen sclerosus overlap syndrome, sharing features of lichen planus and lichen sclerosus. 17
Signs and symptoms edit
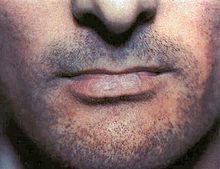
Lichen planus affecting the lower lip.
Although lichen planus can present with a variety of lesions, the most common presentation is as a well-defined area of purple-coloured, itchy, flat-topped papules with interspersed lacy white lines Wickham s striae. This description is known as the characteristic 6 Ps of lichen planus: planar flat-topped, purple, polygonal, pruritic, papules, and plaques. 9 This rash, after regressing, is likely to leave an area of hyperpigmentation that slowly fades. That said, a variety of other lesions can also occur. 8
Cutaneous lichen planus edit
Cutaneous lichen planus on the shin.
Lichen planus involving the nails.
Variants of cutaneous lichen planus are distinguished based upon the appearance of the lesions and/or their distribution. 18 Lesions can affect the:
Extremities face, dorsal hands, arms, and nape of neck. a This is more common in Middle Eastern countries in spring and summer, where sunlight appears to have a precipitating effect. 15 19 20
Palms and soles
Intertriginous areas of the skin. This is also known as Inverse lichen planus. 15
Nails 21 characterized by irregular longitudinal grooving and ridging of the nail plate, thinning of the nail plate, pterygium formation, shedding of the nail plate with atrophy of the nail bed, subungual keratosis, longitudinal erthronychia red streaks, and subungual hyperpigmentation. 22 A sand-papered appearance is present in around 10 of individuals with nail lichen planus. 21
Scalp. This is also known as lichen planopilaris, acuminatus, follicular lichen planus, and peripilaris, 23 characterised by violaceous, scaly, pruritic papules. Scalp lichen planus can cause scarring alopecia if it is untreated. 9 20 24
Hair. This variant causes inflammation of hair follicles and gradual replacement with scarring. About 10 of people with lichen planus have the scalp or nail variants of the condition. 9
Other variants may include:
Lichen planus pemphigoides characterized by the development of tense blisters atop lesions of lichen planus or the development vesicles de novo on uninvolved skin. 25
Keratosis lichenoides chronica also known as Nekam s disease is a rare dermatosis characterized by violaceous papular and nodular lesions, often arranged in a linear or reticulate pattern on the dorsal hands and feet, extremities, and buttock, and some cases manifests by sorrheic dermatitis like eruption on the scalp and face, also palmo plantar keratosis has been reported. 15 26 27
Lichenoid keratoses also known as Benign lichenoid keratosis, and Solitary lichen planus 15 is a cutaneous condition characterized by brown to red scaling maculopapules, found on sun-exposed skin of extremities. 15 28 Restated, this is a cutaneous condition usually characterized by a solitary dusky-red to violaceous papular skin lesion. 29
Lichenoid dermatitis represents a wide range of cutaneous disorders characterized by lichen planus-like skin lesions. 15 28
Mucosal lichen planus edit
Lichen planus on the lips and the lateral border of the tongue
Lichen planus affecting mucosal surfaces may have one lesion or be multifocal. 30 Examples of lichen planus affecting mucosal surfaces include: 30
Esophageal lichen planus, affecting the esophageal mucosa. This can present with difficulty or pain when swallowing due to oesophageal inflammation, or as the development of an esophageal stricture. It has also been hypothesized that it is a precursor to squamous cell carcinoma of the esophagus. 10 31
Genital lichen planus, which may cause lesions on the glans penis or skin of the scrotom in males, and the vulva or vagina in females. 9 Symptoms may include lower urinary tract symptoms associated with stenosis of the urethra, painful sexual intercourse, and itching. 9 In females, Vulvovaginal-gingival syndrome, is severe and distinct variant affecting the vulva, vagina, and gums, with complications including scarring, vaginal stricture formation, 32 or vulva destruction. 33 The corresponding syndrome in males, affecting the glans penis and gums, is the peno-gingival syndrome. 15 It is associated with HLA-DQB1. 15 34
Oral lichen planus edit
Oral lichen planus also termed oral mucosal lichen planus, 35 is a form of mucosal lichen planus, where lichen planus involves the oral mucosa, the lining of the mouth. This may occur in combination with other variants of lichen planus. 36 Six clinical forms of oral lichen planus are recognized: 36
Reticular, the most common presentation of oral lichen planus, 4 is characterised by the net-like or spider web-like appearance of lacy white lines, oral variants of Wickham s straiae. 36 This is usually asymptomatic. 4
Erosive/ulcerative, the second most common form of oral lichen planus, 4 is characterised by oral ulcers presenting with persistent, irregular areas of redness, ulcerations and erosions covered with a yellow slough. This can occur in one or more areas of the mouth. In 25 of people with erosive oral lichen planus, the gums are involved, described as desquamative gingivitis a condition not unique to lichen planus. This may be the initial or only sign of the condition. 36
Papular, with white papules.
Plaque-like appearing as a white patch which may resemble leukoplakia. 36
Atrophic, appearing as areas. Atrophic oral lichen planus may also manifest as desquamative gingivitis. 36
Bullous, appearing as fluid-filled vesicles which project from the surface.
These types often coexist in the same individual. Oral lichen planus tends to present bilaterally as mostly white lesions on the inner cheek, 4 although any mucosal site in the mouth may be involved. Other sites, in decreasing order of frequency, may include the tongue, lips, gingivae, floor of the mouth, and very rarely, the palate. 4
Generally, oral lichen planus tends not to cause any discomfort or pain, although some people may experience soreness when eating or drinking acidic or spicy foodstuffs or beverages. 36 When symptoms arise, they are most commonly associated with the atrophic and ulcerative subtypes. These symptoms can include a burning sensation to severe pain. 4
Causes edit
The cause of lichen planus is unknown, 8 34 37 but it is not contagious and does not involve any known pathogen. 38 It is thought to be a T cell mediated autoimmune reaction where the body s immune system targets its own tissues. 4 This autoimmune process triggers apoptosis of the epithelial cells. 4 Several cytokines are involved in lichen planus, including tumor necrosis factor alpha, interferon gamma, interleukin-1 alpha, interleukin 6, and interleukin 8. 4 This autoimmune, T cell mediated, process is thought to be in response to some antigenic change in the oral mucosa, but a specific antigen has not been identified. 4
Where a causal or triggering agent is identified, this is termed a lichenoid reaction rather than lichen planus. These may include: 11
Drug reactions, with the most common inducers including gold salts, beta blockers, traditional antimalarials e.g. quinine, thiazide diuretics, furosemide, spironolactone, metformin and penicillamine. 38
Reactions to amalgam metal alloys fillings or when they are removed/replaced, 39
Graft-versus-host disease lesions, which chronic lichenoid lesions seen on the palms, soles, face and upper trunk after several months. 38
Hepatitis, specifically hepatitis B and hepatitis C infection, and primary biliary cirrhosis. 17 38
It has been suggested that lichen planus may respond to stress, where lesions may present during times of stress. Lichen planus can be part of Grinspan s syndrome. citation needed
It has also been suggested that mercury exposure may contribute to lichen planus. 40
Diagnosis edit
Lichen planus lesions are diagnosed clinically by their lichen-like appearance. 8 A biopsy can be used to rule out conditions that may resemble lichen planus, and can pick up any secondary malignancies. 41
Histopathology edit
Micrograph of lichen planus. H E stain.
Lichen planus has a unique microscopic appearance that is similar between cutaneous, mucosal and oral. A Periodic acid-Schiff stain of the biopsy may be used to visualise the specimen. Histological features seen include: 42
thickening of the stratum corneum both with nuclei present parakeratosis and without orthokeratosis. Parakeratosis is more common in oral variants of lichen planus.
thickening of the stratum granulosum
thickening of the stratum spinosum acanthosis with formation of colloid bodies also known as Civatte bodies, Sabouraud bodies that may stretch down to the lamina propria.
liquefactive degeneration of the stratum basale, with separation from the underlying lamina propria, as a result of desmosome loss, creating small spaces Max Joseph spaces.
Infiltration of T cells in a band-like pattern into the dermis 4 hugging the basal layer.
Development of a saw-tooth appearance of the rete pegs, which is much more common in non-oral forms of lichen planus.
Differential diagnosis edit
The differential diagnosis for OLP includes:
Other oral vesiculo-ulcerative conditions such as Pemphigus vulgaris and Benign mucous membrane pemphigoid
Lupus erythematosus, with lesions more commonly occur on the palate and appear as centrally ulcerated or erythematous with radiating white striae. In contrast, OLP and lichenoid reactions rarely occur on the palate, and the striae are randomly arranged rather than radial. 43
Chronic ulcerative stomatitis
Frictional keratosis and Morsicatio buccarum chronic cheek biting
Oral leukoplakia
Oral candidiasis
Treatment edit
There is no cure for lichen planus, 4 and so treatment of cutaneous and oral lichen planus is for symptomatic relief or due to cosmetic concerns. 4 8 41 When medical treatment is pursued, first-line treatment typically involves corticosteroids, 8 and removal of any triggers. 39 Without treatment, most lesions will spontaneously resolve within 6–9 months for cutaneous lesions, 8 and longer for mucosal lesions 42
Many different treatments have been reported for cutaneous lichen planus, however there is a general lack of evidence of efficacy for any treatment. 14 44 Treatments tend to be prolonged, partially effective and disappointing. 14 First-line treatments may include retinoids such as Acitretin, or corticosteroids 8 14 44
A variety of other therapies are also used if these are unsuccessful. These include oral corticosteroids, vitamin D3 analogues, antibiotics such as Dapsone, hydroxychloroquine and Cyclosporin, some anti-coagulants, which. and psoralen plus ultraviolet-A. 8 14 44
Cosmetic treatments may include laser surgery, cryotherapy, and phototherapy. 14 44
Reassurance that the condition is benign, elimination of precipitating factors and improving oral hygiene are considered initial management for symptomatic OLP, and these measures are reported to be useful. 4 Treatment usually involves topical corticosteroids such as betamethasone, clobetasol, dexamethasone, and triamcinolone and analgesics, or if these are ineffective and the condition is severe, the systemic corticosteroids may be used. Calcineurin inhibitors such as pimecrolimus, tacrolimus or cyclosporin are sometimes used. 4
Prognosis edit
In contrast to cutaneous lichen planus, lichen planus lesions in the mouth may persist for many years, 41 and tend to be difficult to treat, with relapses being common. 34 Atrophic/erosive lichen planus is associated with a small risk of malignant transformation, 41 and so people with OLP tend to be kept on long term review to detect any potential change early. Sometimes OLP can become secondarily infected with Candida organisms. citation needed
Epidemiology edit
The overall prevalence of lichen planus in the general population is about 0.1 - 4. 9 It generally occurs more commonly in females, in a ratio of 3:2, and most cases are diagnosed between the ages of 30 and 60, but it can occur at any age. 9 45
Oral lichen planus is relatively common, 34 It is one of the most common mucosal diseases. The prevalence in the general population is about 1.27-2.0, 4 41 and it occurs more commonly middle aged people. 4 OLP in children is rare. About 50 of females with oral lichen planus were reported to have undiagnosed vulvar lichen planus. 9
History edit
Lichen planus was first reported in 1869 by Erasmus Wilson. 42
Notes edit
Cutaneous lichen planus affecting the extremities is also known as Lichen planus actinicus, Actinic lichen niditus, Lichen planus atrophicus annularis, Lichen planus subtropicus, Lichen planus tropicus, Lichenoid melanodermatitis, and Summertime actinic lichenoid eruption
References edit
a b c Greenberg MS, Glick M, Ship JA 2008. Burket s oral medicine 11th ed.. Hamilton, Ont.: BC Decker. pp. 89–97. ISBN 9781550093452.
Lewis MAO, Jordan RCK 2012. Oral medicine 2nd ed.. London: Manson Publishing. pp. 66–72. ISBN 9781840761818.
Barnes L editor 2009. Surgical pathology of the head and neck 3rd ed.. New York: Informa healthcare. ISBN 9781420091632.
a b c d e f g h i j k l m n o p q r Thongprasom, K; Carrozzo, M; Furness, S; Lodi, G Jul 6, 2011. Interventions for treating oral lichen planus.. The Cochrane database of systematic reviews 7 : CD001168. doi:10.1002/14651858.CD001168.pub2. PMID 21735381.
a b Asch, S; Goldenberg, G March 2011. Systemic treatment of cutaneous lichen planus: an update.. Cutis; cutaneous medicine for the practitioner 87 3 : 129–34. PMID 21488570.
a b Sharma, A; Białynicki-Birula, R; Schwartz, RA; Janniger, CK July 2012. Lichen planus: an update and review.. Cutis; cutaneous medicine for the practitioner 90 1 : 17–23. PMID 22908728.
a b Cheng, S; Kirtschig, G; Cooper, S; Thornhill, M; Leonardi-Bee, J; Murphy, R Feb 15, 2012. Interventions for erosive lichen planus affecting mucosal sites.. The Cochrane database of systematic reviews 2: CD008092. doi:10.1002/14651858.CD008092.pub2. PMID 22336835.
a b c d e f g h i Limited, Therapeutic Guidelines 2009. Therapeutic guidelines. Version 3. ed.. North Melbourne, Vic.: Therapeutic Guidelines. pp. 254–255, 302. ISBN 978-0-9804764-3-9.
a b c d e f g h i Usatine, RP; Tinitigan, M Jul 1, 2011. Diagnosis and treatment of lichen planus. American family physician 84 1 : 53–60. PMID 21766756.
a b Yamada T, Alpers DH; et al. 2009. Textbook of gastroenterology 5th ed.. Chichester, West Sussex: Blackwell Pub. p. 3304. ISBN 978-1-4051-6911-0.
a b Treister NS, Bruch JM 2010. Clinical oral medicine and pathology. New York: Humana Press. pp. 59–62. ISBN 978-1-60327-519-4.
Freedberg, Irwin M., ed. 2003. Fitzpatrick s dermatology in general medicine 6th ed.. New York, NY: McGraw-Hill. pp. 465–8. ISBN 0-07-138076-0.
a b James, William D.; Elston, Dirk M.; Berger, Timothy G. Andrews Diseases of the skin : clinical dermatology 11th ed.. London: Saunders/ Elsevier. pp. 219–24. ISBN 1-4377-0314-3.
a b c d e f Gorouhi, F; Firooz A; Khatami A; Ladoyanni E; Bouzari N; Kamangar F; Gill JK 2009. Interventions for cutaneous lichen planus. Cochrane Database of Systematic Reviews 4. doi:10.1002/14651858.CD008038.
a b c d e f g h i Bolognia, Jean L.; Jorizzo, Joseph L.; Rapini, Ronald P., eds. 2008. Dermatology 2nd ed.. St. Louis: Mosby/Elsevier. ISBN 1-4160-2999-0.
Freedberg, Irwin M., ed. 2003. Fitzpatrick s dermatology in general medicine 6th ed.. New York, NY: McGraw-Hill. pp. 366, 470–1. ISBN 0-07-138076-0.
a b James, William D.; Elston, Dirk M.; Berger, Timothy G. Andrews Diseases of the skin : clinical dermatology 11th ed.. London: Saunders/ Elsevier. p. 220. ISBN 1-4377-0314-3.
Freedberg, Irwin M., ed. 2003. Fitzpatrick s dermatology in general medicine 6th ed.. New York, NY: McGraw-Hill. p. 466. ISBN 0-07-138076-0.
Freedberg, Irwin M., ed. 2003. Fitzpatrick s dermatology in general medicine 6th ed.. New York, NY: McGraw-Hill. p. 468. ISBN 0-07-138076-0.
a b James, William D.; Elston, Dirk M.; Berger, Timothy G. Andrews Diseases of the skin : clinical dermatology 11th ed.. London: Saunders/ Elsevier. p. 223. ISBN 1-4377-0314-3.
a b Gordon, KA; Vega, JM; Tosti, A Nov–Dec 2011. Trachyonychia: a comprehensive review. Indian journal of dermatology, venereology and leprology 77 6 : 640–5. doi:10.4103/0378-6323.86470. PMID 22016269.
James, William D.; Elston, Dirk M.; Berger, Timothy G. Andrews Diseases of the skin : clinical dermatology 11th ed.. London: Saunders/ Elsevier. p. 781. ISBN 1-4377-0314-3.
Freedberg, Irwin M., ed. 2003. Fitzpatrick s dermatology in general medicine 6th ed.. New York, NY: McGraw-Hill. p. 467. ISBN 0-07-138076-0.
Cevasco NC, Bergfeld WF, Remzi BK, de Knott HR 2007. A case-series of 29 patients with lichen planopilaris: the Cleveland Clinic Foundation experience on evaluation, diagnosis, and treatment. J. Am. Acad. Dermatol. 57 1 : 47–53. doi:10.1016/j.jaad.2007.01.011. PMID 17467854.
Freedberg, Irwin M., ed. 2003. Fitzpatrick s dermatology in general medicine 6th ed.. New York, NY: McGraw-Hill. p. 471. ISBN 0-07-138076-0.
Freedberg, Irwin M., ed. 2003. Fitzpatrick s dermatology in general medicine 6th ed.. New York, NY: McGraw-Hill. p. 472. ISBN 0-07-138076-0.
James, William D.; Elston, Dirk M.; Berger, Timothy G. Andrews Diseases of the skin : clinical dermatology 11th ed.. London: Saunders/ Elsevier. p. 224. ISBN 1-4377-0314-3.
a b Freedberg, Irwin M., ed. 2003. Fitzpatrick s dermatology in general medicine 6th ed.. New York, NY: McGraw-Hill. p. 473. ISBN 0-07-138076-0.
James, William D.; Elston, Dirk M.; Berger, Timothy G. Andrews Diseases of the skin : clinical dermatology 11th ed.. London: Saunders/ Elsevier. p. 639. ISBN 1-4377-0314-3.
a b Ebrahimi, M; Lundqvist, L; Wahlin, YB; Nylander, E October 2012. Mucosal lichen planus, a systemic disease requiring multidisciplinary care: a cross-sectional clinical review from a multidisciplinary perspective. Journal of lower genital tract disease 16 4 : 377–80. doi:10.1097/LGT.0b013e318247a907. PMID 22622344.
Chandan, VS; Murray, JA; Abraham, SC June 2008. Esophageal lichen planus. Archives of pathology laboratory medicine 132 6 : 1026–9. doi:10.1043/1543-2165 2008 132 1026:ELP 2.0.CO;2. PMID 18517264.
Panagiotopoulou, N; Wong, CS; Winter-Roach, B April 2010. Vulvovaginal-gingival syndrome.. Journal of obstetrics and gynaecology : the journal of the Institute of Obstetrics and Gynaecology 30 3 : 226–30. doi:10.3109/01443610903477572. PMID 20373919.
Schlosser, BJ May–Jun 2010. Lichen planus and lichenoid reactions of the oral mucosa.. Dermatologic therapy 23 3 : 251–67. doi:10.1111/j.1529-8019.2010.01322.x. PMID 20597944.
a b c d Nico, MM; Fernandes, JD; Lourenço, SV Jul–Aug 2011. Oral lichen planus.. Anais brasileiros de dermatologia 86 4 : 633–41; quiz 642–3. PMID 21987126.
Alam, F; Hamburger, J May 2001. Oral mucosal lichen planus in children.. International journal of paediatric dentistry / the British Paedodontic Society and the International Association of Dentistry for Children 11 3 : 209–14. PMID 11484471.
a b c d e f g Scully C 2008. Oral and maxillofacial medicine : the basis of diagnosis and treatment 3rd ed.. Edinburgh: Churchill Livingstone. pp. 192–199. ISBN 9780702049484.
Roopashree, MR; Gondhalekar, RV; Shashikanth, MC; George, J; Thippeswamy, SH; Shukla, A November 2010. Pathogenesis of oral lichen planus--a review.. Journal of oral pathology medicine : official publication of the International Association of Oral Pathologists and the American Academy of Oral Pathology 39 10 : 729–34. doi:10.1111/j.1600-0714.2010.00946.x. PMID 20923445.
a b c d Davidson s principles and practice of medicine. 21st ed.. Edinburgh: Churchill Livingstone/Elsevier. 2010. pp. 1265–1266. ISBN 978-0-7020-3085-7. first1 missing last1 in Authors list help
a b Issa, Y; Brunton, PA; Glenny, AM; Duxbury, AJ November 2004. Healing of oral lichenoid lesions after replacing amalgam restorations: a systematic review.. Oral surgery, oral medicine, oral pathology, oral radiology, and endodontics 98 5 : 553–65. doi:10.1016/j.tripleo.2003.12.027. PMID 15529127.
Dunsche A, Frank MP, Lüttges J, et al. April 2003. Lichenoid reactions of murine mucosa associated with amalgam. The British Journal of Dermatology 148 4 : 741–8. doi:10.1046/j.1365-2133.2003.05229.x. PMID 12752133.
a b c d e Kerawala C, Newlands C, ed. 2010. Oral and maxillofacial surgery. Oxford: Oxford University Press. pp. 412–413. ISBN 978-0-19-920483-0.
a b c Scully, C.; El-Kom, M. 1 July 1985. Lichen planus: review and update on pathogenesis. Journal of Oral Pathology and Medicine 14 6 : 431–458. doi:10.1111/j.1600-0714.1985.tb00516.x.
Odell EW Editor 2010. Clinical problem solving in dentistry 3rd ed.. Edinburgh: Churchill Livingstone. pp. 159–162, 192. ISBN 9780443067846.
a b c d Cribier, B; Frances, C; Chosidow, O December 1998. Treatment of lichen planus. An evidence-based medicine analysis of efficacy.. Archives of dermatology 134 12 : 1521–30. doi:10.1001/archderm.134.12.1521. PMID 9875189.
Yu TC, Kelly SC, Weinberg JM, Scheinfeld NS March 2003. Isolated lichen planus of the lower lip. Cutis 71 3 : 210–2. PMID 12661749.
External links edit
Wikimedia Commons has media related to Lichen planus.
Lichen planus at DMOZ
Retrieved from https://en.wikipedia.org/w/index.php.title Lichen_planus oldid 691644096 Classification
Categories: Lichenoid eruptionsConditions of the mucous membranesHepatitis C virus-associated diseasesAutoimmune diseasesOral mucosal pathology.
Circular Red Rash. Besides being a cause of cosmetic concern, skin rashes could also be accompanied by redness and itching. The following Buzzle write-up provides.
Acrokeratosis paraneoplastica of Bazex; Acroosteolysis; Bubble hair deformity; Disseminate and recurrent infundibulofolliculitis; Erosive pustular dermatitis of the scalp.
There are many different causes behind the occurrence of a circular red rash on the skin. Some of the genuine reasons that cause a circular read rash have been enlisted in the following article. To know more about, read on
As mentioned above, there can be several reasons for the development of such a rash on the skin. Circular red rashes that occur on the human skin can be classified into two types, namely the rashes that appear as a result of allergies, which can be treated with the help of allergy relief solutions and the rashes that appear as a result of infections, where microbes are responsible for occurrence of the rash.
Rash as a Result of Allergies
Circular red rashes occur often in the form of poison ivy rash or due to contact with plants and animals, that have a tendency to secrete substances that are poisons and abrasive in nature and tend to harm the human skin. The rash that occurs in such cases, tends to be very painful and prominent. The best solution in such a scenario is to consult a doctor. It is advisable not to wash the rash, as it might further spread the poison. Relief creams that provide a temporary soothing are available in most of the first aid kits, and also as over-the-counter medication. You may consult your chemist or physician to get to know the exact medication. Such rashes also appear as a result of some inherited disorders, conditions or allergies such as eczema, which can be treated with appropriate eczema lotions. In case of allergies, the rash is easily curable and the body itself tends to develop counter measures.
Rash as a Result of Infection
A rash that occurs as a result of infection and foreign bodies, is more severe and painful than the allergic rashes. Medical assistance in the form of antibiotics, disinfectants and artificial antibodies is required to curb the rash. The following are some of the causes:
1. Lyme Disease: Lyme disease is caused as a result of a bacterium known as Borrelia burgdorferi. The Borrelia burgdorferi, is a bacterium that infects the human body and is communicated by parasitic arachnids, which are small parasitic insects, often referred to as ticks. A drawback is that the Lyme disease is not detected very early in most of the cases due to its symptoms, which are very similar to many other medical conditions and diseases. The common symptoms of Lyme disease include, fatigue, fever, stiff muscles, joint pain and in general symptoms, that resemble those of flu. The symptom that indicates that the illness is Lyme disease is the raised circular red rash on chest, arm or legs or for that matter anywhere on the skin. More on Lyme Disease Symptoms in Humans.
2. Ringworm: Another known cause for the occurrence of a raised circular red rash is infection of ringworm. The ringworm in reality is not a worm, but is a kind of fungal infection. The raised circular rash is easily cured with the help of antifungal creams and some mild antibiotics.
3. Diabetes: Though diabetes is not a disease but a disorder, it tends to act like a non-contagious disease in some cases. This can be observed in cases where the small blood vessels near the skin change and result into a condition that is known as Diabetic Dermopathy. A rash on the legs often appears when a person is affected by Dermopathy. In many cases, the rash turns brown in color. The rash that occurs as a result of Dermopathy does not hurt at all and no treatment is required. This condition is experienced frequently by many diabetics due to the change in the nature of blood vessels.
Thus, the best way to get rid of a circular read rash is to consult a doctor as soon as possible. The circular red rash on arms, legs or skin may be also caused by poisonous substances, hence, the early the remedy, the better would be the cure. Stay Healthy, Stay Safe, Stay Rash Free.
Browse and search the Indie DB article listing to read the the inside scoop direct from indie game development teams including exclusive news, previews, interviews.
Read about home remedies for dry skin and dry skin treatments. Also read how to cure dry skin naturally with proven home remedies.
Read Detailed feature on Homeopathic remedies for Skin rashes, Skin itching and irritation. Information on Homeopathic treatment for rash.
